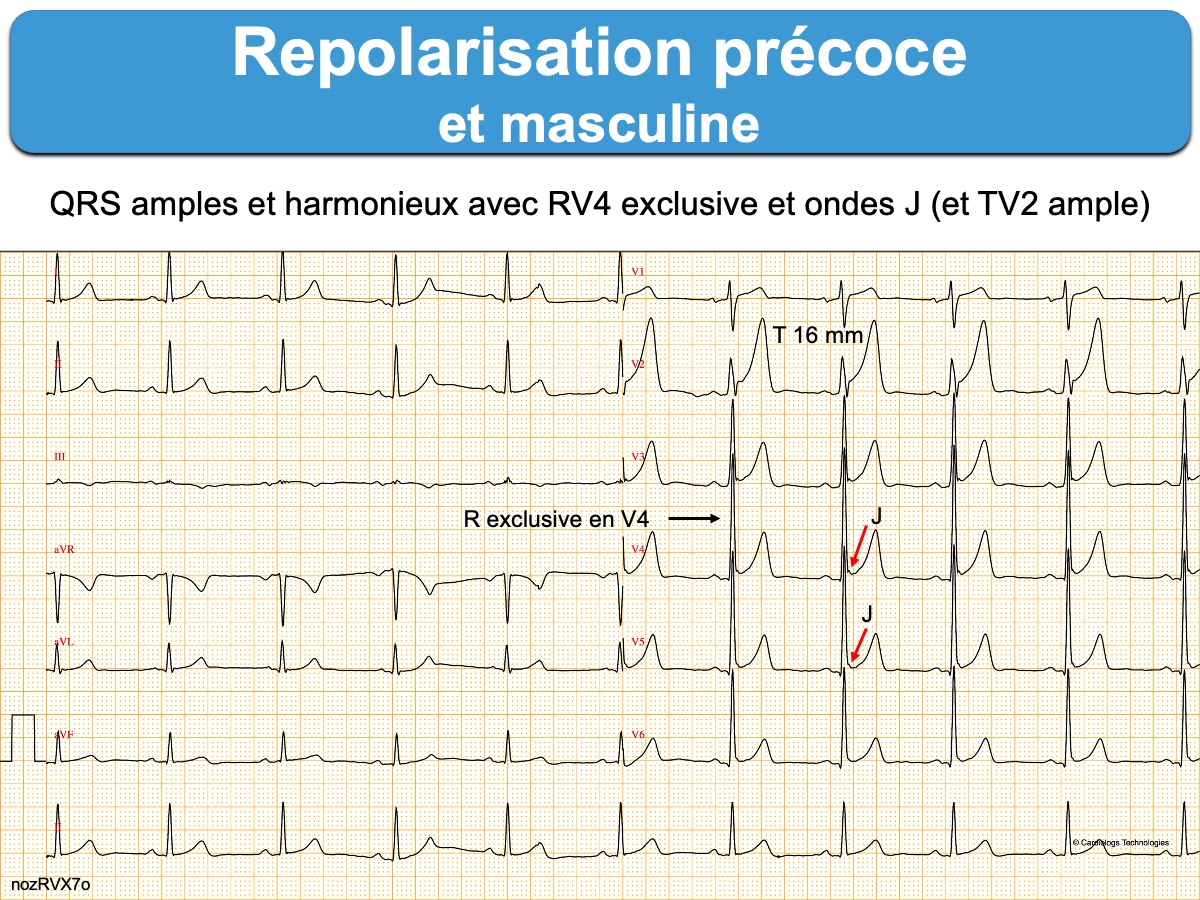
Variante normale de repolarisation de type masculine caractérisée par un sus-décalage de ST ascendant et des ondes T amples, prédominant dans les dérivations précordiales droites (V2-V3) [1].
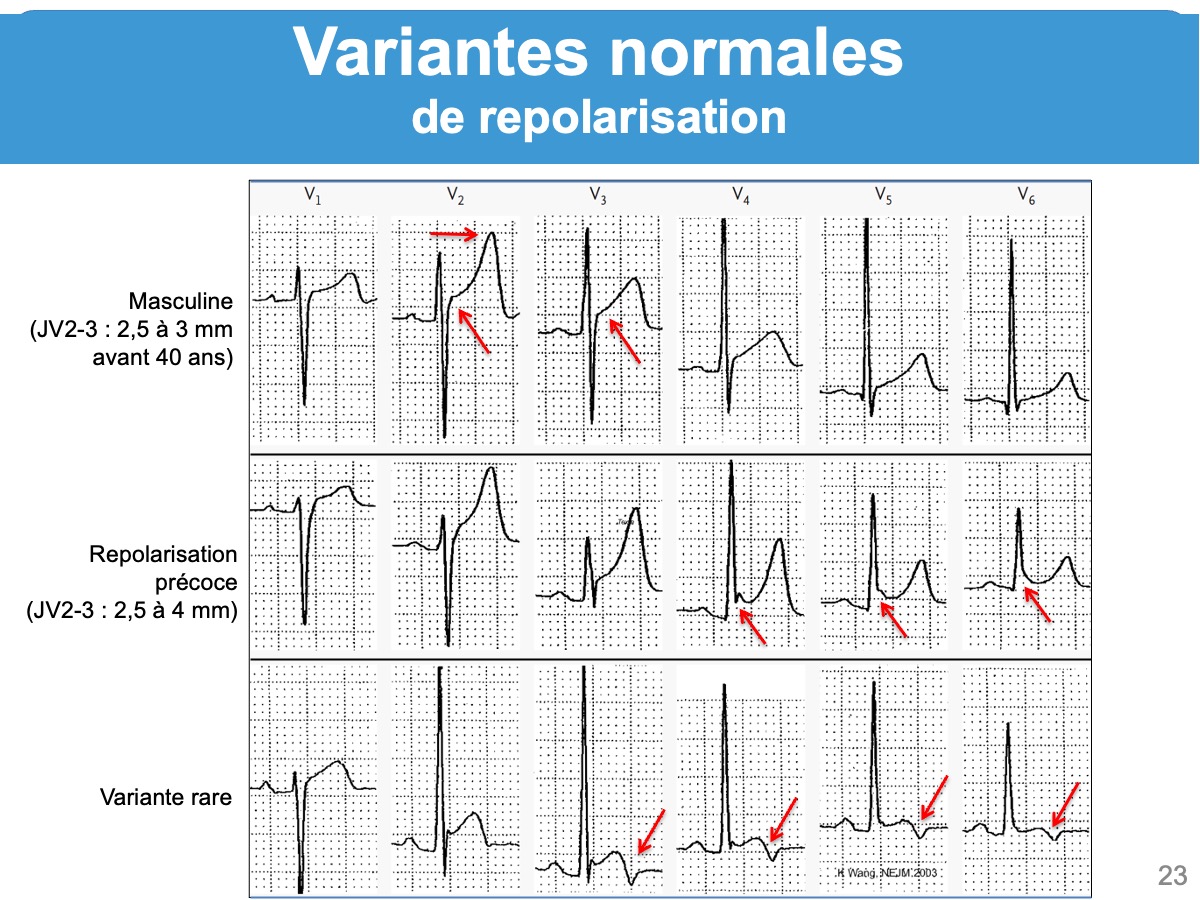
Cette variante se rencontre chez 90% des jeunes hommes, en particulier d’origine africaine, et elle s’atténue avec l’âge (male pattern) [1][3]. Ce n’est donc pas une variante chez l’homme jeune, mais un aspect normal.
Aspect ECG
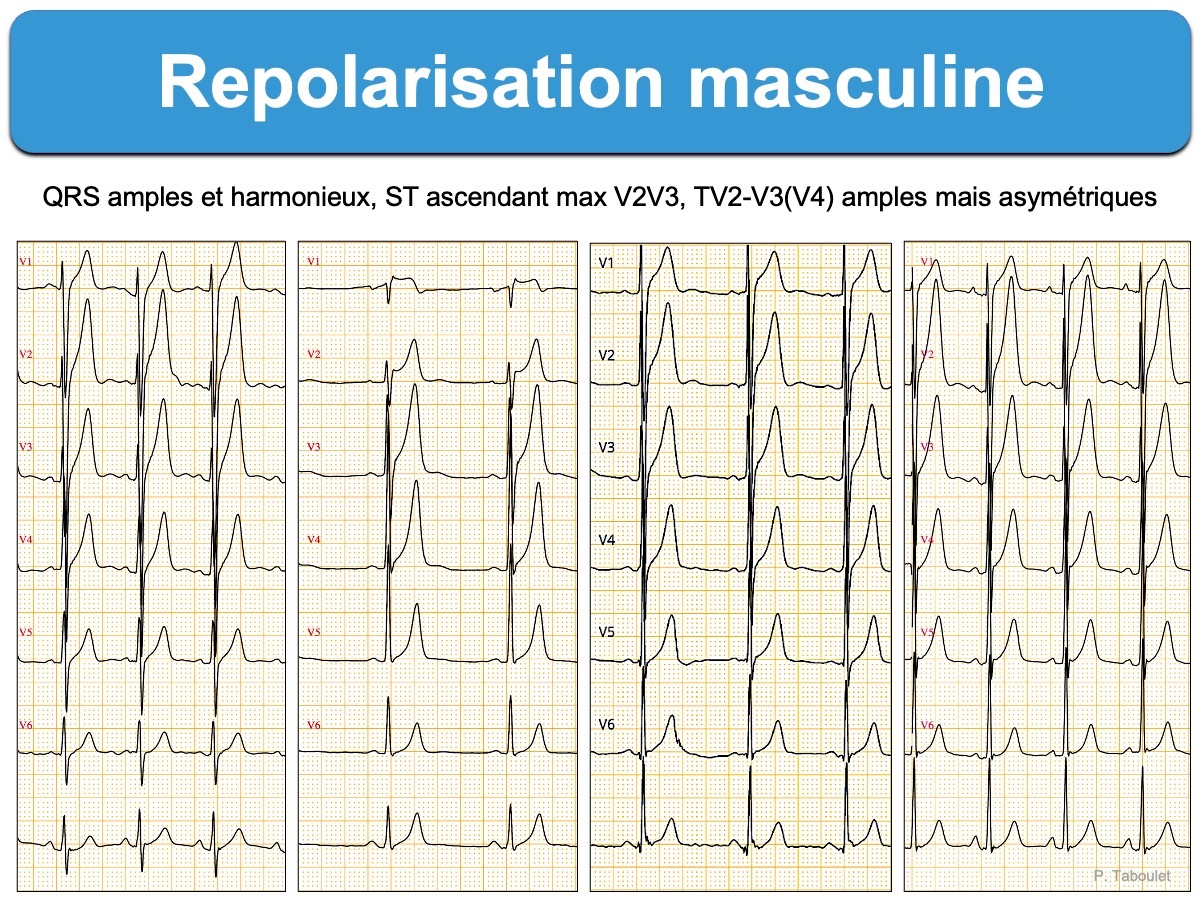
Les complexes QRS sont amples, avec une croissance rapide des ondes R de V1 à V4 et une zone de transition généralement déviée à droite (V1-V2 ou V2-V3). Il en résulte parfois une onde R exclusive en V4.
- Le point J est surélevé parfois de 3 mm en V2-V3 (en particulier chez les hommes jeunes en bonne santé originaire d’Afrique), mais non crocheté et il n’y a pas d’onde J [3].
- Le segment ST est rapidement ascendant* et concave en regard des ondes T amples [2].
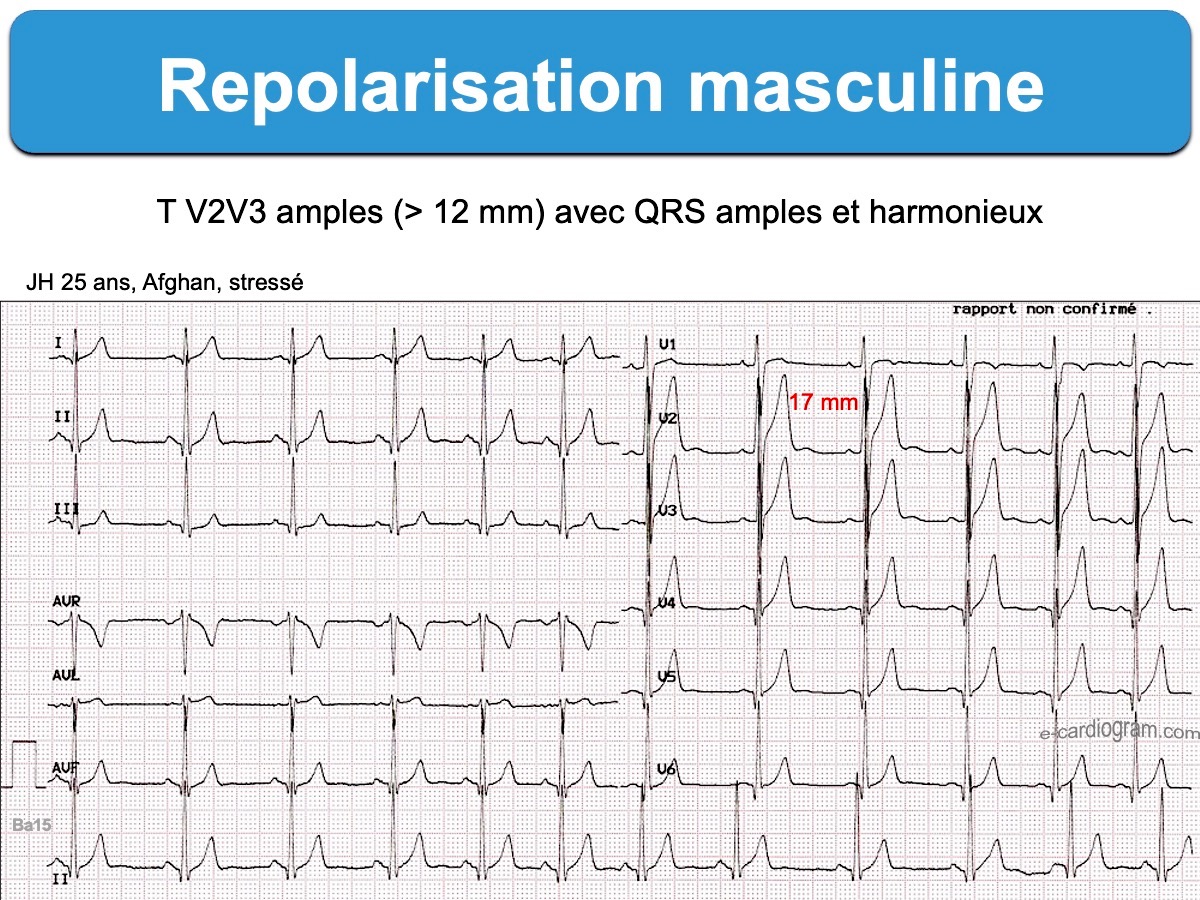
- Les ondes T sont amples dans le précordium (max 16-20 mm en V2-V3, voir ici) et asymétriques à leur base [2]. L’onde T est souvent d’autant plus ample que le nadir de S est profond [3].
- L’intervalle QT est normal ou plus court que chez des sujets contrôles [3].
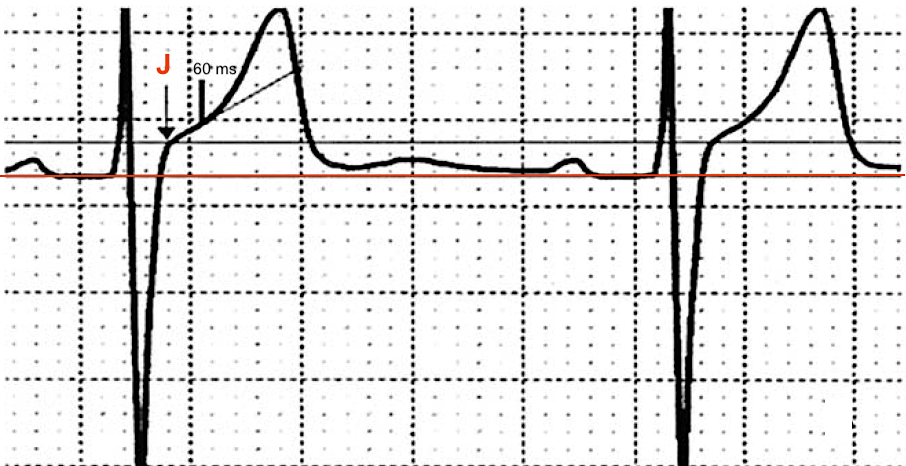
Le caractère “rapidement ascendant” est exprimé par un angle ≥ 20 degré entre la ligne Q-Q et le point J à + 60 ms [2].
Diagnostics différentiels
- Repolarisation précoce (ondes J). L’association avec une repolarisation masculine est fréquente. L’élévation du point J peut atteindre 4 mm.
- Syndrome coronaire aigu ST+ (QRS modifiés par l’ischémie, miroir, trouble du rythme…). L‘indice de Smith peut aider à le reconnaitre [4]. Lire ici.
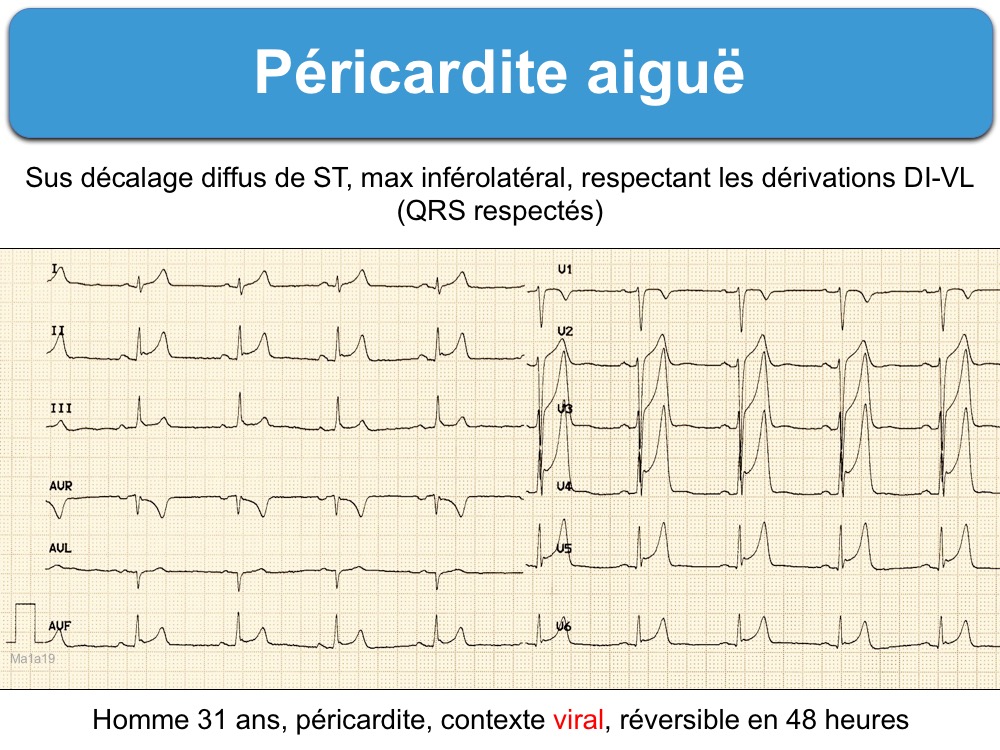
- Péricardite (QRS respectés avec progression harmonieuse des ondes R en précordiales, pas de miroir, sous décalage de PQ, parfois microvoltage…)
L’analyse complète de l’ECG, les tracés antérieurs et successifs – couplés à la clinique – permettent le plus souvent de trancher.
Blog de SW Smith
- Chest pain and Very Large T-waves
- A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chest pain
[1] Macfarlane PW, Antzelevitch C, Haissaguerre M, et al. The Early Repolarization Pattern: A Consensus Paper. J Am Coll Cardiol. 2015;66(4):470-7.
[2] Surawicz B, Parikh SR. Prevalence of male and female patterns of early ventricular repolarization in the normal ECG of males and females from childhood to old age. J Am Coll Cardiol 2002; 40:1870-6. (téléchargeable)
To measure the ST angle we drew a line that was parallel to the Q–Q line at the level of the J point and a line connecting the J point with a point situated 60 ms after the J point. The angle between these two lines represents the ST angle. The pattern was considered as male when the J point was ≥ 0.1 mV in at least one of the four leads and when the ST angle was ≥ 20° in at least one of these leads (V1 à V4)
[3] Wang K, Asinger RW, Marriott HJ.. ST-segment elevation in conditions other than acute myocardial infarction. NEJM. 2003;349(22):2128-35. (téléchargeable)
In a recent study of normal electrocardiograms from 529 men, the prevalence of ST-segment elevation of at least 1 mm in one or more of leads V1 through V4 was 93 percent in the men who were 17 to 24 years old
In some healthy young people, especially in black men, the ST segment is elevated by 1 to 4 mm in the midprecordial leads as a normal variant (Kambara H, Phillips J. Long-term evaluation of early repolarization syndrome (normal variant RS-T segment elevation). Am J Cardiol. 1976 Aug;38(2):157-6. )
In contrast, about 20 percent of normal electrocardiograms from women had ST-segment elevation of 1 mm or more, and this prevalence remained unchanged regardless of the women’s ages.
The deeper the S wave, the greater the ST-segment elevation — a relation that is often observed in patients with left ventricular hypertrophy
[4] Smith SW, Khalil A, Henry TD, et al. Electrocardiographic differentiation of early repolarization from subtle anterior ST-segment elevation myocardial infarction. Ann Emerg Med. 2012;60(1):45-56.
Smith SW, Zvosec DL, Sharkey SW, et al. The ECG in acute MI: an evidence-based manual of reperfusion therapy. Philadelphia, PA, USA: Lippincott Williams and Wilkins; 2002
Si la moyenne des amplitudes de l’onde R de V2 à V4 est inférieure à 5 mm, il s’agit presque certainement d’un infarctus. Si cette moyenne est supérieure à 5 mm, il s’agit probablement d’une repolarisation précoce. Le seuil de 5 mm donne une sensibilité pour MI d’environ 70%, mais une spécificité supérieure à 95%.[1] If the mean R-wave amplitude from V2-V4 is less than 5 mm, then it is almost certainly MI. If greater than 5 mm, it is probably BER. A cutoff of 5 mm gives a sensitivity for MI of about 70%, but a specificity of greater than 95%.