Aslanger et coll. ont identifié en 2020 un aspect ECG spécifique (Aslanger pattern) qui prédit un infarctus aigu dans le territoire inférieur par occlusion de l’artère coronaire droite ou de la circonflexe malgré un sus-décalage de ST en DIII et uniquement en DIII [1]. Le pronostic est moins bon qu’un infarctus incluant un ST+ ≥ 1 mm dans au moins les deux dérivations DIII et VF.
Ce pattern est considéré comme un équivalent ST+, c’est-à-dire un infarctus par occlusion coronaire aiguë sans que soit atteint le seuil d’élévation du point J de 1 mm dans deux dérivations du territoire inférieur (cf. Infarctus inférieur). Le sus-décalage isolé en DIII s’explique par la coexistence d’une ischémie sous-endocardique (ST-) dans le territoire opposé au territoire inférieur (subendocardial ischaemia) en rapport avec l’atteinte plurivasculaire.
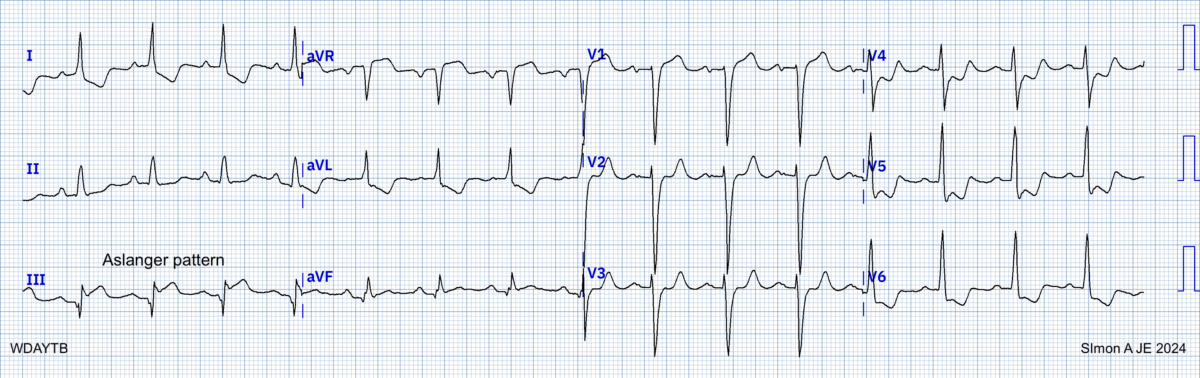
Le pattern d’Aslanger
Il comprend trois signes [1]
1) Sus-décalage isolé de ST en dérivation DIII (pas en VF)
2) ST+ en V1 > V2
3) ST- dans une ou plusieurs dérivations V4-V6, avec une onde T positive/terminale
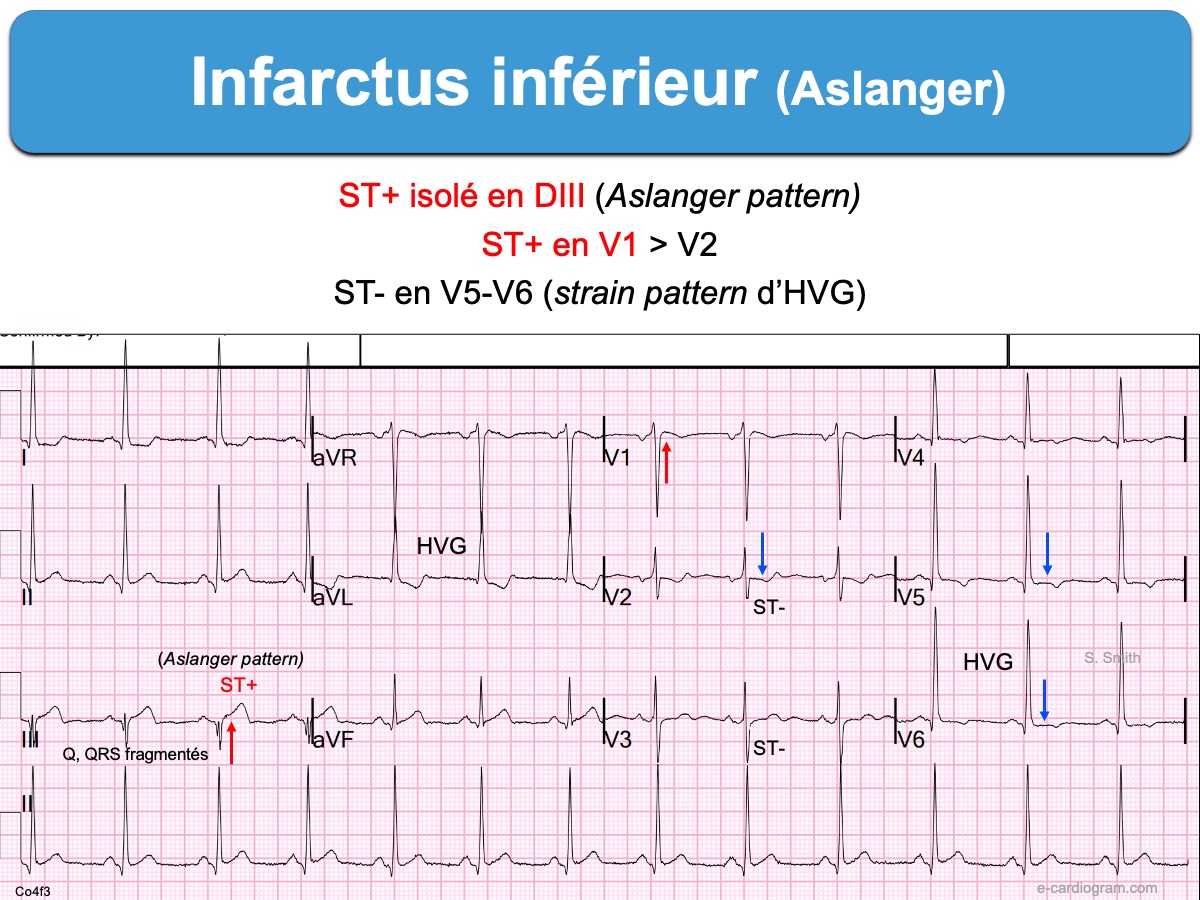

Le ST- est relativement diffus. Il affecte V4-V6 et DI-VL et DII. Le ST- en DII s’oppose au ST+ en DIII ce qui annule le décalage de ST en VF car VF = 1/2 (DII + DIII) [3][4].
Le ST+ se voit mieux en -VL et en -DI et aussi VR et V1.
L’aspect peut être très subtil pour un œil non averti.
Le pattern d’Aslanger a été observé chez 6,3 % (61/966) des 1000 patients de la cohorte des infarctus non ST+ avec coronarographie de référence et 0,5 % (5/1000) des patients sans infarctus du myocarde. Les patients avaient une maladie multivasculaire, un infarctus de taille plus grande et un pronostic moins bon que les patients qui avaient un infarctus inférieur avec un sus-décalage de ST académique (ST+ ≥ 1 mm dans deux des trois dérivations DII-DIII-VF) [1].
L’origine de ce pattern/syndrome remonte en fait à 1995 dans l’étude rétrospective de Sclarovsky S et al [2] qui signale la présence d’un sus-décalage de ST < 1 mm en VF and environ 8% des cas d’infarctus inférieur.
Blog de S. Smith (anglais)
- Aslanger Pattern
- Un pattern subtil et tardif –> March 15, 2015. avant la publication conjointe avec Aslanger: chest-pain-what-do-you-see-on-ecg
La suite est réservée aux membres et stagiaires du site.
Se connecter | Devenir membre | Devenir stagiaire